
Improving Emergency Department Cash Flow Via Lean Six Sigma
Emergency Department Project Overview
Industry
Health Care
Company
A not-for-profit hospital system
Results
$600,000 and increased E.D. patient flow
Tools Used
Six Sigma DMAIC
Timeline
Six months
Problem Statement
A not-for-profit hospital system noticed that many of its patients were routinely leaving the E.D. (emergency department) without providing complete insurance verification information or making appropriate financial arrangements. This information was critical to ensure a timely and accurate billing process and cash flow.
In addition, the hospital system was only collecting 30% of the charges billed for E.D. patients that were treated and released and less than $300 per day in co-pays.
Business Case
The business case for this project was clear. An eight-week analysis of E.D. gross revenue charges identified that $356,000 was not collectable because of incomplete patient registrations.
This translated to an average of $177,000 per month in lost revenue. The collection ratio in the E.D. was 31%, which meant there was a net revenue potential of $55,000 per month ($177,000 x 31%), translating to a potential $660,000 net revenue per year.
The hospital was collecting less than $300 per day in co-pays, with a potential
to collect $1,200 per day. Increasing collections by $900 per day would translate to collecting an additional $330,000 per year.
Project Goals
The hospital’s goal was to increase the collection ratio to 40% within six months by securing each patient’s financial responsibility information before they were discharged. It sought a clearly defined and consistently applied process to capture this information for every patient, every time.
In addition, the hospital wanted to increase the amount of cash collected from patients at the time of service from $300 per day to $1,200 per day.
Project Team
A multidisciplinary project team was selected to improve the billing process in the E.D. The team consisted of representatives from finance, medical staff, legal services, support services, and nursing.
Project Scope
The project scope was unsecured patient accounts. The beginning boundary for the project was the time a patient arrived in the E.D. The ending boundary was when the patient was discharged from the E.D. and financial responsibility was secured.
The team selected the DMAIC process as its improvement method. A Six Sigma DMAIC project is defined as a project that eliminates a chronic problem that is causing patient dissatisfaction, defects, costs of poor quality, or other deficiencies in performance.
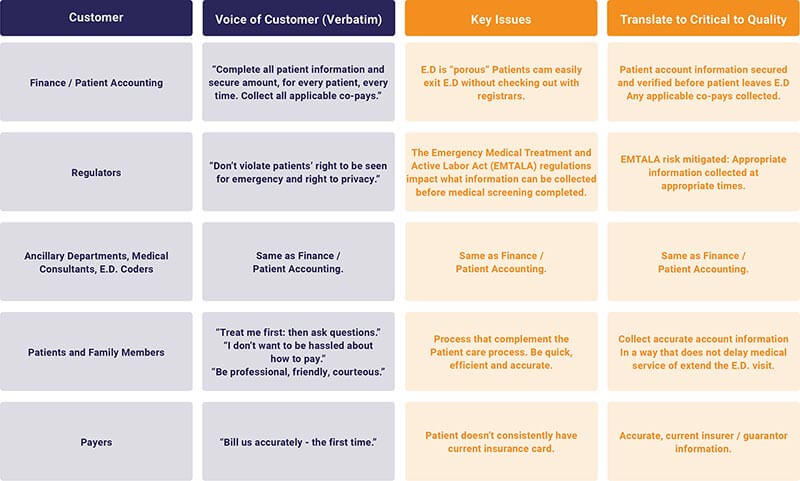
Understanding the Needs of the Emergency Department's Audiences
In order for the hospital to appropriately meet the needs of its internal and external customers, it had to accurately measure and understand their issues. Once the key issues were identified, the team translated them into “critical-to-quality” (CTQ) needs.
Emergency Department's Current Process Capability
Using the previous year’s data, the hospital outlined its current process capabilities. There were total charges of roughly $71 million and 65,756 hospital visits. The median billed charge per visit was $1,080. As previously calculated in its eight-week analysis of E.D. gross revenue charges, there were $356,000 in unbilled accounts. This translated to 41 defects
per week ($356,000/$1080/8 weeks).
The estimated current process capability was:
- Sigma Level: 3.4 (short term)
- % defects: 3%
The target sigma level was 4.0 or greater, meaning there would be less than one incomplete account per day.
What are the gap areas?
After understanding and analyzing its current process maps, the team concluded that:
- The most important element of quick registration was the accurate identification of the patient.
- Bedside registration added to patient wait times. Missed opportunities were occurring when the patients were in the main waiting room.
- Bedside registration did not work well when the patient wait times were minimal.
- Checkout at a patient’s bedside was awkward and inefficient for both patients and registrars.
- The registrar’s toolset did not support bedside registration.
- The registration and checkout processes were highly dependant on the patient care process and patient flow
Where are the relationships?
Using a cause-and-effect diagram, the hospital team identified some of the major factors that were contributing to unsecured accounts. They included:
- People – Probable root causes included each person’s level of training and experience, possible bad habits, and which registrars were available.
- Patients – Probable root causes included the severity of the patient’s physical state, as well as their lucidity. Each patient’s primary language was also a factor, along with whether or not he or she had their insurance card on hand.
- Facility – Probable root causes included the location of the registration station(s), as well as the number of unsecured exits from the E.D. In addition, there was no defined checkout process or location within the E.D.
- Regulatory – Probable root causes included meeting EMTALA, HIPAA, and JCAHO/CMS requirements.
- Tools – Probable root causes included the proximity of computers, access to wireless Internet, access to the online eligibility system, and access to Medipac.
- Process – Probable root causes included inconsistency in registration and the checkout process.
Emergency Department's Activity
The hospital system tracked the total E.D. visits by day of the week and time of the day over an 18-month. It found that patients generally arrived in a predictable pattern, regardless of the day. Peak times were highest on Mondays and lowest on Saturdays. With this knowledge, the hospital could appropriately develop staffing patterns that matched patient arrival patterns.
Severity, Probability, Detection
Left Without Being Seen (LWBS) was the primary reason for unsecured accounts. The majority of accounts were not secured because of patients who left from the lobby without being seen. Over a third of the accounts were not secured because the patient left before being checked out.
- Co-pays were being collected on just more than 3% of the patients in the E.D.
- The majority of E.D. patients did not have co-pays due. The top three reasons co-pays were not collected were: 1. Self-pay patients were not asked for a deposit. 2. Patients requested to be billed 3. The hospital was simply not asking.
- There was a lack of a defined, consistent checkout process; patients were “escaping” from the E.D. before account information had been collected or verified.
- For patients who were seen, the providers or nurses were discharging them before the registrar could return to the room or simply losing track of them after they had seen a provider.
- Communication was poor between clinical staff and registrars.
- Registrars needed help in knowing when the patient was available to interview and verify the information.
- There were problems with patient flow; patients were leaving from several exits.
What was contributing to unsecured patient accounts?
Utilizing Juran’s Pareto Analysis, the hospital team was able to identify the vital few Xs that were contributing to the unsecured patient accounts. They found that:
- Patient activity impacted the unsecured accounts: Higher patient volumes were predictive of a greater number of unsecured accounts.
- Patient flow in the E.D.: There were many ways for patients to exit undetected and there was no defined checkout process. Checkout at a patient’s bedside was inconsistent.
- Collected patient account information was not integrated into the patient care process: Providers were discharging patients without involving the registrars and not telling the registrars when patients were waiting for test results.
- Patients who left without being seen were a major source of unsecured accounts: No attempts were being made to collect registration information for patients who were waiting in the lobby.
- Process was not designed for transparency and self-control: Registrars had no visual cues to know when the process was in control or out of control.
Emergency Department's Implementation & Control Plan
Once detail-level designs were created and approved, the project team developed an implementation and control plan that included:
- Bedside registration of emergency patients using wireless data entry.
- Central intake/registration of non-emergent patients (level 3-5).
- A hardwired checkout process where all patients are to be escorted to the checkout desk.
- Integrated clinical care process and registration.
- Visual alerts to improve communication between providers and registrars when patients were available to complete registration.
- Process transparency and operational metric reporting.
- Training for registrars and clinical staff of the process changes and new data collection tools. ▪ Adding a back-up workstation to the checkout desk for peak periods of patient flow.
- Collecting data on key metrics at the end of every shift. ▪ Instructing hospital registrars to always ask for co-pays and inform patients of their financial obligation.
Results
The number of incomplete accounts for patients leaving the Emergency Department declined from 4% per month to less than 1% per month within a six-month time frame. This was a statistically significant difference and represented an improvement in the number of accounts the hospital could now bill and expect to collect on.
This meant the hospital had successfully reached its target sigma level of 4.0, meaning there would be less than one incomplete account per day. The annualized financial impact and increase in collections because of fewer incomplete accounts was $535,000. The improvement in co-pays was an additional $73,000 annually. The total annualized benefit was approximately $600,000.
Other benefits from the Six Sigma implementation included:
- An enhanced checkout experience for patients leaving the E.D.
- All patients directed to check-out.
- Improved patient flow – all patients see a nurse on check-in.
- Improved staffing pattern and assignments of registrars at the hospital.
- More clearly defined roles for hospital personnel.
Transform Your Business
Get in touch with us for more information on how we can help your organization attain sustainable results, and start your journey towards world class quality.
Related Resources





